|
|
|||||||||||||
Dissector Answers - Pelvis & Perineum |
|||||||||||||
Learning Objectives:
Upon completion of this session, the student will be able to:
- Trace the continuity of the abdominal peritoneum with that of the pelvic cavity, and identify the peritoneal pouches of the pelvic floor in both sexes.
- Identify the superficial features of the external genitalia.
- Describe the normal position and relationships of all organs of the reproductive tracts in both sexes and the role of each in reproductive processes.
- Describe the broad ligament and differentiate its parts.
- Identify the ovary and discuss the functional significance of its ligaments.
- Demonstrate the uterine tube and its subdivisions.
- Identify the uterus and its subdivisions and demonstrate the continuity of its lumen with that of the uterine tubes and the vagina.
- Differentiate between the internal and external os of the cervix.
- Identify the vagina, and note the angle formed at its junction with the uterus.
- Trace the entire course of the ductus deferens and identify its ampulla; note its relationship to the ureter.
- Identify the seminal vesicle and demonstrate the formation and course of the ejaculatory duct.
- Identify the prostate gland and describe the special features of the prostatic urethral wall.
- Identify the testis, its coverings, and tubules, and account for the difference in location between gonads in the two sexes.
- Demonstrate the epididymis and its subdivisions.
- Describe the formation of the two sciatic foramina. List the muscles, nerves, and vessels which pass through each.
- Demonstrate the origins of the piriformis and obturator internus muscles and describe two specializations of the obturator fascia.
- Identify the pelvic diaphragm and differentiate its components.
- Trace the branching pattern of the internal iliac vessels in each sex, identifying branches by their relationships to pelvic organs or wall structures.
- Demonstrate the formation of the sacral plexus, its relationship to the piriformis muscle and gluteal vessels, and its pelvic splanchnic nerves.
- Identify and describe the inferior hypogastric (pelvic) plexus and its connections to the superior hypogastric plexus via the hypogastric nerves.
- Identify and describe the sacral sympathetic trunks and the sacral sympathetic nerves.
- Trace the sympathetic and parasympathetic nerve supply to any pelvic organ, listing the location of the preganglionic cell body, the course of preganglionic fibers, the location of the postganglionic cell body, and the course of postganglionic fibers, as well as the sensory supply of the pelvic organs.
- Trace the lymphatic drainage of the genital organs in both sexes.
- Trace the skeletal and ligamentous boundaries of the perineum, and define the anal and urogenital triangles.
- Describe the position and boundaries of the ischioanal fossa.
- Describe the structure, contents, and course of the pudendal canal.
- Trace the branching pattern of the internal pudendal vessels and the pudendal nerve.
- Differentiate between the internal and external anal sphincters in structure and function.
- Differentiate between male and female urethrae.
- Identify the components of the external genital organs and give the homologues in each of both sexes.
- Describe structure and function of the erectile bodies.
- Trace the nerve and blood supply to the external genital organs.
- Trace the lymphatic drainage of the perineum.
Learning Objectives and Explanations:
1. Trace the continuity of the abdominal peritoneum with that of the pelvic cavity, and identify the peritoneal pouches of the pelvic floor in both sexes. (W&B 533-534, N 360, 361, 362, 363, 371, TG 6-07A, 6-07B, 6-08A, 6-08B, 6-11, 6-13)2. Identify the superficial features of the external genitalia. (W&B 519-522, N 351, 377, 382, 387, 390, 398, TG 6-02, 6-25A, 6-25B, 6-31)The peritoneum continues from the abdominal cavity into the pelvic cavity, but does not entirely invest the pelvic viscera. In the female, the peritoneum:
- extends from the anterior abdominal wall to the superior surface of the bladder, not drooping low enough to catch the anterior surface
- sweeps over the fundus and covers part of the posterior surface of the bladder
- jumps from the posterior surface of the bladder to the anterior (vesicle) surface of the uterus
- sweeps superiorly, to the fundus of the uterus, contacting the uterine tubes
- the space created by the peritoneum sweeping down the back of the bladder, over to the uterus, and up the front of the uterus is the vesicouterine pouch
- continues around the fundus of the uterus, and over the uterine tubes, to the posterosuperior (intestinal) surface of the uterus
- the "doubling" of the peritoneal layers as they hang on either side of the uterine tubes creates the broad ligaments
- jumps from the uterus to cover the anterior portion of the rectum, starting about 2/3 of the way down the rectum
- continues up the rectum, investing the sides as well as it reaches the superior 1/3, attaching to the posterior body wall
- the space created by the peritoneum sweeping across the uterus, jumping to the rectum, and beginning to travel up the front of the rectum is the rectouterine pouch
3. Describe the normal position and relationships of all organs of the reproductive tracts in both sexes and the role of each in reproductive processes. (W&B 543-553, N 360, 362, 369, 370, 371A, 371B, 378, 382A, 382B, 383, 399, 400, 402, 404A, 404B, 352, 359, 361A, 361B, 362, 363, 365, 384A, 384B, TG 5-34, 6-07A, 6-07B, 6-08A, 6-08B, 6-09A, 6-09B, 6-10A, 6-10B, 6-11, 6-12, 6-14, 6-15, 6-17, 6-23, 6-29, 6-31)Sorry to cop out and paste in the tables, but there is little connectivity or functionality that needs to be explained. It is pretty much a "these are the things you should know about" situation.
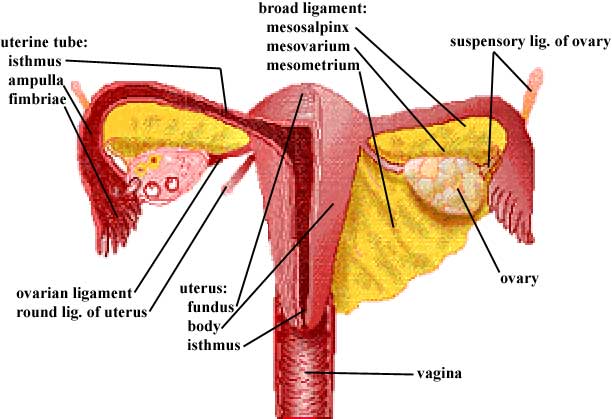
4. Describe the broad ligament and differentiate its parts. (W&B 547-548, N 371, TG 6-07, 6-08, 6-11, 6-12)These diagrams will be useful here, and for the remaining objectives in this session:
Female:
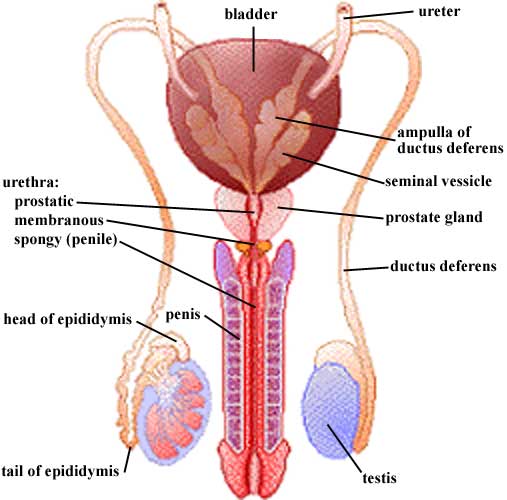
Male:
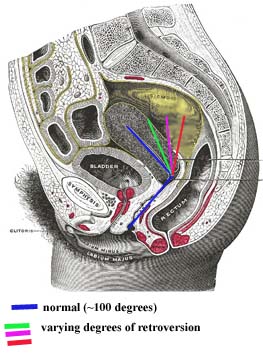
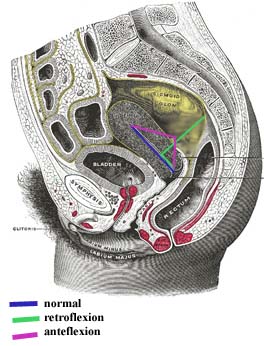
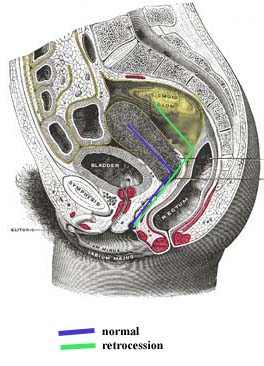
Female: The uterus is more or less horizontal in orientation. It actually lies upon the bladder, so its vesical surface is partially anterior but mostly inferior. Its intestinal surface faces the pelvic cavity. Deviations from this "flopped over the bladder" position can happen. Terms that are "________version" refer to the angle between the long axis of the uterus and the long axis of the vagina. This angle is usually about 100 degrees. Cases where the uterus stands more vertically, and therefore that angle approaches 180 degrees, are called RETROversion. Terms that are "________flexion" refer to the long axis of the body of the uterus as compared to the long axis of the uterine cervix. The long axis of a normal body of the uterus is relatively horizontal, while in the cervix the axis turns partially vertical. With RETROflexion the uterus is actually flopped back, away from the bladder. With ANTEflexion, the uterus is kinked, with a marked angle between the long axis of its body and the long axis of its cervix. (A slight bit of anteflexion is very normal.) Cases where the entire uterus, cervix and all, is moved posteriorly are called retrocession. The vagina is longer here.
Images from "Anatomy of the Human Body" by Henry Gray are provided by:
The uterine (fallopian) tubes attach somewhat laterally to the uterus. They reach toward the ovaries, but are not "officially" attached to them. The fimbriae of the uterine (fallopian) tubes come closest to contacting the ovary. The ovaries themselves are the female gonads. They lie against the pelvic walls.
The female gametes (ova, eggs) mature in the ovaries. In the normal case, one egg is released per month from one ovary or the other. This egg is actually released into the pelvic cavity, but the waving motion of the fimbriae help guide the egg into the uterine tube. The tube is the usual site of fertilization of the egg by sperm, then the newly formed zygote travels to the uterus. It is the job of the uterus to provide an environment for growth of the embryo.
Male: The normal positioning of things in the male is pretty straightforward. The testes are suspended outside the body within the scrotum. A ductus deferens (vas deferens) leads from each testis, through the inguinal canal, around to the posterior part of the bladder. Here they dilate, forming the ampulla of the ductus deferens. Also on the posterior aspect of the bladder lie the seminal vesicles. On each side, the ductus deferens and seminal vesicle join to form the ejaculatory duct, which dumps into the prostatic portion of the urethra. From there, the urethra travels through the penis to its external opening.
The male gametes (sperm) develop within the tissue of the testes. They leave the testes proper as immature gametes. They finish their maturation and are stored in the epidiymis. When needed, they quickly traverse the entire length of the ductus deferens to the ejaculatory duct. At this junction with the seminal vesicles, important materials are added to the semen, the fluid surrounding the sperm. The prostate gland also makes a contribution to the semen. From here the whole mix is sent down the urethra, through the penis, and out of the body.
5. Identify the ovary and its two ligaments and tell the functional significance of both ligaments. (W&B 547-548, N 369, TG 6-07, 6-08, 6-11, 6-12)The broad ligament is a section of peritoneum, like a mesentery, which extends from the pelvic walls to the uterus and uterine (fallopian) tubes. Its three parts are continuous with each other, making it difficult to discern at their junctions. The mesosalpinx is the peritoneum that covers the uterine tube and hangs below it to meet with the mesovarium. The mesovarium is the peritoneum covering the ovary and ovarian ligament, extending like a shelf posteriorly from the mesosalpinx. (If you squint at the diagram in #11, you'll see a ridge of peritoneum running along the top of each ovary.) The mesometrium is the rest of the broad ligament - all of the peritoneum directly connected to the uterus and extending toward the lateral abdominal wall. (Greek, metra = uterus, from meter (mother);
6. Demonstrate the uterine tube and its subdivisions. (W&B 547-548, N 371, TG 6-07, 6-08, 6-11, 6-12)The suspensory ligaments of the ovaries are peritoneal folds covering the ovarian neurovascular supply as the vessels pass over the pelvic brim and into the pelvis to reach the ovary. The suspensory ligament conducts ovarian arteries and veins, nerves, and lymphatics to the ovary. The "ovarian ligament" proper is a round cord which attaches the ovary to the uterus just below the entrance of the uterine tube into the uterus. The ovarian ligament, a remnant of a portion of the gubernaculum, is within the mesovarium.
7. Identify the uterus and its subdivisions and demonstrate the continuity of its lumen with that of the uterine tubes and the vagina. (W&B 548-551, N 371, TG 6-07, 6-08, 6-11, 6-12)The uterine tube extends laterally about 10 cm from the uterus to the ovary. It has three parts:
- isthmus: the constricted part adjacent to the uterus
- ampulla: the widest and longest part, extending laterally to the infundibulum from the isthmus
- infundibulum: the funnel-like terminus, with fringed processes called fimbriae that contact the ovary.
8. Differentiate between the internal and external os of the cervix. (W&B 551-553, N 371, TG 6-11, 6-12)The lumen of the uterus is continuous on both sides with the lumens of the uterine tubes. It is continuous inferiorly with the lumen of the vagina. It is divided into four parts:
9. Identify the vagina, and note the angle formed at its junction with the uterus. (W&B 551-553, TG 6-08, 6-11, 6-12, 6-13)The tapered neck or cervix of the uterus is traversed by the cervical canal. Above, it is continuous with the cavity of the body of the uterus at the internal os. Below, at a depression on the vaginal portion of the cervix, the external os opens into the cavity of the vagina.
10. Trace the entire course of the ductus deferens and identify its ampulla; note its relationship to the ureter. (W&B 545, N 361A, 361B, 363, 384A, 384B, 390, TG 6-10, 6-31A, 6-31B)The vagina is muscular, but not as much as the uterus. The angle between its long axis and the long axis of the uterus is about 100 degrees in normal cases. Other cases can occur, as described in #12 above.
11. Identify the seminal gland and demonstrate the formation and course of the ejaculatory duct. (W&B 545-546, N 361A, 361B, 384A, 384B, TG 6-10)The ductus deferens is an unbelievable 45 cm long! It starts in the tail of the epididymis, ascends as part of the spermatic cord, traverses the inguinal canal, emerges from the deep inguinal ring, passes lateral to the inferior epigastric artery, ascends obliquely across the external iliac arteries, goes over to the back side of the bladder and descends on the fundus medial to the ureter and seminal vesicles. The ductus deferens joins the duct of the seminal vesicle at the prostate to form the ejaculatory duct. The most distal portion of the ductus is the ampulla, which is tortuous and dilated. ("Ductus deferens" literally means "deferent vessel", which means "vessel that shows respect and esteem due a superior or an elder".)
12. Identify the prostate gland and describe the special features of the prostatic urethral wall. (W&B 546-547, N 361, 384A, 384B, TG 6-10)The seminal glands lie lateral to the ampulla of the ductus deferens on the posterior side of the bladder. Their ducts join the ductus deferens to form the ejaculatory ducts. They are similar in structure to the ampulla of the ductus.
13. Identify the testis, its coverings, and tubules, and account for the difference in location between gonads in the two sexes. (W&B 431-433, 544-545, N 387, 388, 390, TG 5-10, 6-31, 6-32)The prostate gland sits under the bladder, with the ampulla of the rectum posterior to it. (The rectovesical septum is between the two.) The base of the gland, which is the TOP, is continuous with the bladder wall. The ejaculatory ducts enter the prostate posterosuperiorly and run to the prostatic urethra.
The prostatic urethra is three to four centimeters long. The urethral crest is a ridge within it, and the prostatic sinuses are valleys on either side of the crest. The little ducts of the prostate gland empty into these sinuses.
The seminal colliculus is a rounded eminence in the middle of the prostatic urethra. A small slit in this structure leads to a very small blind pouch in the prostate. This pouch is the prostatic utricle (or "vagina masculina"), the male homologue of the uterus and vagina, i.e. the remnant of the Mullerian duct system. Near the mouth of the prostatic utricle, the two ejaculatory ducts empty into the prostatic urethra. (Latin, utriculus = little leather bag)
14. Demonstrate the epididymis and its subdivisions. (W&B 544, N 390, TG 6-32)The testes are covered by a tough, fibrous coat called the tunica albuginea testis. Superficial to that they are invested by two layers of tunica vaginalis testis, much like the pleura or peritoneum. (This structure is actually derived from the processus vaginalis of the peritoneum.) The visceral layer of the tunica vaginalis testis almost completely covers each, only being absent where the testis attaches to the epididymis. The parietal layer of the tunica vaginalis testis is more extensive yet, extending for a short distance along the spermatic cord. (Latin, tunica albuginea = white membrane, covering)
The gonads have a similar path of development in both sexes, up to a point. That point is when the ovaries try to start descending and find that the uterus is in the way. So, they stay where they are.
15. Describe the formation of the two sciatic foramina. List the muscles, nerves, and vessels which pass through each. (W&B 570-571, N 352, 503, TG 3-28, 6-06)The epidiymis is a coil of tubes that lies on the posterior aspect of the testis. (The total length of each tube, if uncoiled, is 15-20 feet.) It is divided into three parts: (Greek, epi = upon, didymos = testicle, twin)
- head of the epididymis: the largest mass of coils, located on the superoposterior part of the testis
- body of the epididymis: inferior to the head, the coiling here is not as pronounced
- tail of the epididymis: the smallest, most inferior portion, which connects to the ductus deferens
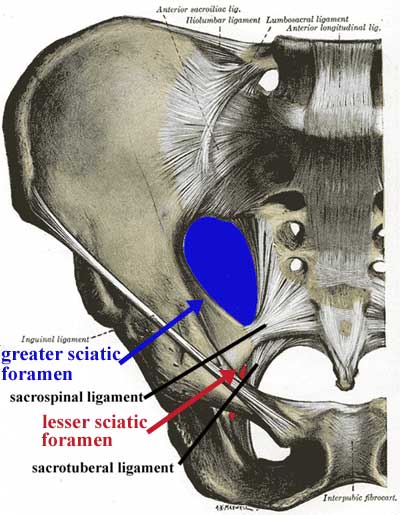
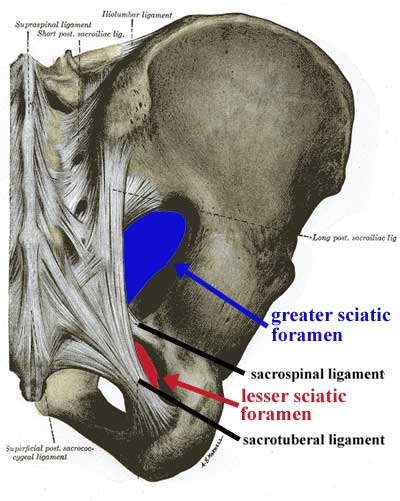
16. Demonstrate the origins of the piriformis and obturator internus muscles and describe two specializations of the fascia of the latter. (W&B 564-565, N 367A, 367B, 369, 503, TG 3-28, 6-21A, 6-21B, 6-22)This is something that only makes sense in three dimensions. You must look at a pelvis from your bone box or in the lab, and figure out where these ligaments are going. Luckily, they are named in a very logical way. These anterior and posterior views might help.
Images from "Anatomy of the Human Body" by Henry Gray are provided by:
The sacrotuberal ligament connects the sacrum to the the ischial tuberosity. With the pelvis in the correct position, it runs mostly inferolaterally from the sacrum to the tuberosity, and only slightly anteriorly. The sacrospinal (sacrospinous) ligament connects the sacrum to the ischial spine. With the pelvis in correct anatomical position, it runs anterolaterally from the sacrum to the ischial spine, but does not deviate much in the superior-inferior axis.
These ligaments, along with the greater sciatic notch and the lesser sciatic notch, make up the greater sciatic foramen and the lesser sciatic foramen, respectively.
greater sciatic foramen: bounded anteriorly and superiorly by the posterior border of the hip bone (greater sciatic notch), posteriorly by the sacrotuberal ligament, and inferiorly by the sacrospinal ligament. The piriformis muscle passes through this opening, as do these nerves and vessels:
- superior to piriformis muscle: superior gluteal vessels and nerve
- inferior to piriformis muscle: inferior gluteal vessels and nerve, the sciatic nerve, the posterior femoral cutaneous nerve, and the nerve to the quadratus femoris muscle - also, the internal pudendal vessels and nerve and the nerve to the obturator internus muscle leave the pelvis via this opening, but enter the perineum through the lesser sciatic foramen (see below)
lesser sciatic foramen: bounded anteriorly by the ischial tuberosity, superiorly by the ischial spine and sacrospinal ligament, and posteriorly by the sacrotuberal ligament. It transmits the tendon of the obturator internus muscle - also, the nerve to the obturator internus muscle and the internal pudendal vessels and nerve, which left the pelvis via the greater sciatic foramen, re-enter the pelvis (in the case of the nerve to the obturator internus muscle) or the perineum (in the case of the internal pudendal vessels and nerve) via the lesser sciatic foramen
17. Identify the pelvic diaphragm and differentiate its components. (W&B 565-566, N 367A, 367B, 368, 369, 370, TG 6-23, 6-21A, 6-21B, 6-22, 6-23)The piriformis muscle takes origin from the anterior surfaces of S2 to S4, both between and lateral to the sacral foramina. It exits the pelvis via the greater sciatic foramen, inserting on the greater trochanter of the femur in order to rotate the thigh laterally. (Latin, piriformis = pear-shaped)
The obturator internus muscle takes origin from the whole bony rim of the obturator foramen, the inner surface of the obturator membrane, and a large area of the inner surface of the ischium. It leaves the pelvis (or, more correctly, its tendon does so) via the lesser sciatic foramen to insert onto the greater trochanter of the femur in order to rotate the thigh laterally. Its fascia has two specializations. First, there is a strong band that stretches between the spine of the ischium and the superior pubic ramus. This is the arcus tendineus levator ani, which gives origin to the levator ani muscles. The other specialization is the obturator membrane, which nearly covers the entire obturator foramen, only leaving space for the obturator nerves and vessels to exit.
18. Trace the branching pattern of the internal iliac vessels in each sex, identifying branches by their relationships to pelvic organs or wall structures. (W&B 553-559, N 398, 400, 401, 402, 403A, 403B, 404A, 404B, 405, TG 6-17A, 6-17B, 6-29A, 6-29B)The pelvic diaphragm is shaped like a bowl, with bony attachments at the pubic symphysis and the coccyx. Between those bones, it is attached to a thickening of the obturator internus muscle fascia called the arcus tendineus levator ani. It is made of two muscles, one of which is divided into 3 (or 4) parts.
Muscle Origin Insertion Action coccygeus ischial spine side of the coccyx and lower sacrum elevates the pelvic floor levator ani posterior surface of the body of the pubis, arcus tendineus levator ani, ischial spine anococcygeal raphe and coccyx elevates the pelvic floor iliococcygeus (part of levator ani) arcus tendineus levator ani and the ischial spine anococcygeal raphe and the coccyx elevates the pelvic floor pubococcygeus (part of levator ani) posterior aspect of the superior pubic ramis coccyx elevates the pelvic floor puborectalis (part of levator ani) posterior aspect of the body of the pubis unites with the puborectalis m. of other side posterior to the rectum draws the distal rectum forward and superiorly pubovaginalis (sometimes listed, part of levator ani) posterior aspect of the body of the pubis fascia of the vagina and perineal body draws the vagina forward and superiorly Furthermore, the diaphragm includes the inferior fascia and the superior fascia. The inferior fascia is an extension of the obturator internus fascia and is continuous with the fascia of the external sphincter ani muscle. The superior fascia is an extension of the transversalis fascia. The two layers are continuous in the urogenital hiatus.
19. Demonstrate the formation of the sacral plexus, its relationship to the piriformis muscle and gluteal vessels, and its pelvic splanchnic nerves. (W&B 559-561, N 402, 409, 410, 412, 415, 416, 417, 497, 499A, 499B, TG 3-25A, 3-25B, 6-17, 6-18, 6-19)The abdominal aorta splits into two common iliac arteries at the level of the L4 vertebra. The common iliac arteries each give off external and internal branches at about the level of the disk between L5 and S1. The external iliac arteries continue outside of the pelvis to supply the lower extremities. The internal iliac arteries enter the pelvic cavity, and generally divide into anterior and posterior divisions to supply pelvic viscera, the buttocks, some of the medial thigh, and the perineum.
The internal iliac artery system is one of the most variable in the body. Therefore, don't try to memorize the exact order of the branches. Just know which division they usually come from and any spatial relationships that are important.
Each posterior division only gives off branches to muscle and body wall. These include:
- superior gluteal artery: supply to gluteus maximus muscle, gluteus medius muscle, gluteus minimus muscle, and hip joint
- iliolumbar artery: supply to iliacus muscle, psoas major muscle, and quadratus lumborum muscle via iliac and lumbar branches
- lateral sacral arteries (usually two per side): supply to sacrum, sacral nerve rootlets, meninges, and adjacent muscles
Each anterior division gives off branches to muscle and body wall, as well as branches to pelvic viscera. Branches to muscle and body wall include:
- inferior gluteal artery: supplies gluteus maximus muscle and the hip joint
- obturator artery: supply to the medial thigh and hip via pubic, acetabular, anterior, and posterior branches
- internal pudendal artery: the primary blood supply to the perineum. It supplies the anus, muscles of the superficial and deep perineal spaces, clitoris or penis, and the posterior aspect of the labium majus or scrotum via numerous branches. (Latin, pudere = to be ashamed)
Branches to pelvic viscera from the anterior division include:
- middle rectal artery: supply to the middle portion of the rectum
- umbilical artery: supply to the superior part of the bladder by giving off the superior vesical arteries, and, in males, to the ductus deferens via the artery of the ductus deferens. (Distal to those branches, the umbilical artery is not patent, and becomes the medial umbilical ligament.)
- inferior vesical artery: supply to lower part of the bladder and to the vagina or prostate. It anastomoses with, and sometimes is a branch of, the middle rectal artery.
- uterine artery (in females): supply to uterus, uterine tube, and upper vagina. The latter two are via tubal and vaginal branches.
- vaginal artery (in females): supply to a major portion of the vagina. It anastomoses with, and sometimes is a branch of, the uterine artery.
For more than you ever wanted to know about anatomical variation, the University of Iowa has a great site, an "Illustrated Encyclopedia of Human Anatomic Variation". Here is a quick and dirty link to the section on internal iliac arteries.
The internal ilac vein on each side receives tributaries that roughly correspond to the branches of the internal iliac artery. These include the superior and inferior gluteal veins, the obturator vein, the internal pudenadal vein, the lateral sacral vein, the middle rectal vein, the vesical vein, prostatic vein (in males), and/or uterine and vaginal veins (in females). The iliolumbar vein drains directly into the common iliac vein on each side.
20. Identify and describe the inferior hypogastric (pelvic) plexus and its connections to the superior hypogastric plexus via the hypogastric nerves. (W&B 562-564, N 409, 410, 412, TG 8-18, 8-19, 8-20, 8-21)Images from "Anatomy of the Human Body" by Henry Gray are provided by:
The sacral plexus proper includes contributions from L4 through part of S4. (Also shown here is the coccygeal plexus, which includes the rest of S4, S5, and the coccygeal nerve.) All of the contributing nerves, except S4, divide into anterior (shown yellow above) and posterior (shown yellow with black shading above) branches.
sciatic nerve: actually two separate nerves that are usually fused together (though in some cases they are not) - the tibial nerve, from anterior branches of L4 through S3, and the common fibular (peroneal) nerve, from the posterior branches of L4 through S2. The sciatic nerve runs under the piriformis muscle, emerging at its inferior border. It travels through the greater sciatic foramen, and on into the thigh. The sciatic nerve provides motor innervation to the hamstrings (posterior thigh muscles) and all of the muscles in the leg and the foot.
superior gluteal nerve: from posterior branches of L4 through S1. Travels through the greater sciatic foramen superior to the piriformis muscle, and moves laterally between the gluteus medius muscle and the gluteus minimus muscle. Provides motor innervation to gluteus medius muscle, gluteus minimus muscle, and tensor fascia lata muscle.
inferior gluteal nerve: from the posterior branches of L5 through S2. Travels through the greater sciatic foramen inferior to the piriformis muscle, and travels for a short distance deep to the gluteus maximus muscle but superficial to the sciatic nerve. It provides the sole motor innervation of the gluteus maximus muscle.
nerve to quadratus femoris muscle: from the anterior branches of L4 through S1. Travels through the greater sciatic foramen inferior to the piriformis muscle. Provides motor innervation to quadratus femoris and inferior gemellus muscles.
nerve to obturator internus muscle: from the anterior branches of L5 through S2. Travels through the greater sciatic foramen inferior to the piriformis muscle, but then loops back around to re-enter the pelvis through the lesser sciatic foramen. Provides motor innervation to the obturator internus and superior gemellus muscles.
posterior femoral cutaneous nerve: from the anterior branches of S2 and S3 and the posterior branches of S1 and S2. Travels through the greater sciatic foramen inferior to the piriformis muscle, and lies alongside the sciatic nerve. It provides sensory innervation to the skin of the back of the thigh in addition to the skin of the lower and lateral buttocks (through gluteal branches) and the perineum (via perineal branches).
pudendal nerve: from the anterior branches of S2 through S4. Travels through the greater sciatic foramen inferior to the piriformis muscle, but then loops back around to enter the perineum through the lesser sciatic foramen, entering the pudendal canal. Provides motor innervation to the muscles of the perineum, and is the primary sensory innervation to the genitalia. (Latin, pudere = to be ashamed)
perforating cutaneous nerve: from the posterior branches of S2 and S3. Pierces the sacrotuberal ligament to provide sensory innervation to the skin of the medial part of the fold of the buttock.
nerve to piriformis muscle: from posterior branches of S1 and S2. Provides motor innervation to the piriformis muscle.
nerves to coccygeus and levator ani muscles: from anterior branches of S3 and S4. Provide motor innervation to coccygeus and levator ani muscles.
pelvic splanchnic nerves: from the ventral primary rami of S2 through S4. Travel to the inferior hypogastric plexus (see below).
perineal branch of the fourth sacral nerve: from the anterior branch of S4. Descends through the coccygeus muscle and runs anteriorly to the external sphincter ani muscle. Provides motor innervation to this muscle and sensory innervation to the overlying skin.
21. Identify and describe the sacral sympathetic trunks and the sacral splanchnic nerves. (W&B 562-564, N 415, 416, 417, TG 8-18, 8-20)The inferior hypogastric plexus is a major meshwork of nerves that are located on either side of the rectum, cervix, and lateral vagina in the female, or on either side of the rectum, prostate, and seminal vessicles in the male. It receives the following:
hypogastric nerves: from the superior hypogastric plexus. These are the primary ways in which sympathetic neurons reach the hypogastric plexus, and therefore the pelvic viscera.
sacral splanchnic nerves: from the second and/or third ganglia of the sacral sympathetic trunk. These are the secondary ways in which sympathetic neurons reach the hypogastric plexus, and therefore the pelvic viscera.
pelvic splanchnic nerves: from the ventral primary rami of S2 through S4. These are the ways in which parasympathetic neurons reach the hypogastric plexus, and therefore the pelvic viscera and distal colon. (Remember that the parasympathetic part of the autonomic nervous system is the "craniosacral" part. Parasympathetic innervation to most of the gut comes from the "cranio-" half of that, i.e., the vagus nerve. The rest, to colon distal to the splenic flexure and to pelvic viscera, is from the "-sacral" half, via the pelvic splanchnic nerves. See also #7 below.)
Note: So far we have seen thoracic, lumbar, sacral, and pelvic splanchnic nerves. Remember that "splanchnic" really only means that they are going to viscera. It so happens that the first three emerge from sympathetic chain ganglia and carry sympathetic fibers, while the fourth has nothing to do with the sympathetic nervous system. If it helps, i.e. does not confuse you more, just remember that the splanchnic nerves come from the chain ganglia and carry sympathetic fibers, with the exception of the pelvic splanchnic nerves.
22. Trace the sympathetic and parasympathetic nerve supply to any pelvic organ, listing the location of the preganglionic cell body, the course of preganglionic fibers, the location of the postganglionic cell body, and the course of postganglionic fibers, as well as the sensory supply of the pelvic organs. (TG 8-18, 8-19, 8-20, 8-21)The sacral sympathetic trunk is slender, and often has 4 or fewer visible ganglia. The trunks lie on the anterior surface of the sacrum and the origin of piriformis, medial to the anterior sacral foramina, which have the large sacral ventral primary rami emerging laterally. The trunk has gray rami branching laterally to reach these sacral VPR's, and you may see very slender, hair-like sacral splanchnic nerves passing anteriorly onto the sides of the rectum to join the inferior hypogastric plexus.
23. Trace the lymphatic drainage of the genital organs in both sexes. (TG 6-33, 6-34)Sympathetic: The preganglionic cell body is located in the lateral horn of the spinal cord in the thoracolumbar region. Axon travels out of the cord via the spinal nerve to the sympathetic chain ganglion. In the lumbar region, some of the nerves will synapse there and either travel down the chain to the pelvis or out via the lumbar splanchnic nerves. In the former case, they leave the chain in the pelvis, via a sacral splanchnic nerve, to reach the hypogastric plexus. In the latter case, they may reach the hypogastric plexus (the long way) via the superior hypogastric plexus and hypogastric nerves.
Parasympathetic: The preganglionic cell body is located in the lateral horn of the spinal cord in the sacral region. Axon travels out of the spinal cord via S2, S3, or S4 spinal nerves. These give off pelvic splanchnic nerves, which reach the hypogastric plexus. From here the neurons travel to their target, usually synapsing with a postganglionic neuron within the tissue of the target organ.
Sensory: Generally speaking, sensory fibers from pelvic structures touched by peritoneum will follow sympathetic innervation, while sensation from pelvic organs deep to the peritoneum follows parasympathetic supply (pelvic splanchnic nerves). This is sometimes referred to as the "pelvic pain line". Remember, however, that there is an inferior boundary to the region of parasympathetic sensation, such as the pectinate line of the anus where sensation above travels via parasympathetics while below it travels via inferior rectal branches of the pudendal nerve.
24. Trace the skeletal and ligamentous boundaries of the perineum, and define the anal and urogenital triangles. (W&B 519, N 379A, 379B, TG 6-24A, 6-24B)Uterus: The lymphatic collecting vessels of the uterus arise in the subserous plexus; to this plexus the deeper lymphatic channels drain. The lymphatic drainage of the uterus is directed to various node groups, principally on a regional basis:
1) From the body of the uterus, collecting vessels pass lateralward between the layers of the broad ligaments to end in the external iliac nodes.
2) Collecting vessels from the body of the uterus also follow the uterine vessels, terminating in the internal iliac nodes.
3) Lymph vessels from the fundus join ovarian collecting channels and follow the ovarian vessels to the lumbar nodes.
4) A few lymph channels from the fundus and the upper body accompany the round ligaments of the uterus and end in the superficial inguinal nodes.
5) Lymphatic channels from the cervical portion of the uterus end partly in the internal and external iliac nodes but also pass backward under the rectouterine ligament to the sacral and the median common iliac nodes.
Uterine tubes: The lymphatics join the ovarian channels, ending in the lumbar nodes.
Ovaries: The lymphatic drainage of the ovary is by channels which ascend in the suspensory ligament to the lumbar chain of nodes.
Vagina: The lymphatics of the vagina differ regionally. From the upper portion of the vagina the collecting channels join those from the cervix uteri and reach both the external iliac and internal iliac nodes. The middle and lower regions drain particularly along the vaginal vessels to the internal iliac groups. The lowest part of the vagina (below the hymen) drains, as does the perineum, to the superficial inguinal node groups.
Testes: The lymphatics of the testis emerge at the mediastinum and join channels draining the epididymis. The collecting vessels ascend in the spermatic cord, accompany the testicular vessels through the inguinal canal, and terminate in the lumbar chain of nodes at levels below the renal blood vessels.
Ductus deferens and seminal vesicles: The lymphatics of the ductus deferens which arise from parts distal to the brim of the pelvis join the lymphatic vessels of the testis. The lymphatics of the pelvic part of the ductus deferens and of the seminal vesicles pass, with those of the prostate and the bladder, to the internal iliac lymph nodes and the posteromedial nodes of the external iliac group.
Prostate: The lymph vessels are associated with those of the seminal vesicles and the neck of the bladder. They end in the sacral and internal iliac nodes.
25. Describe the position and boundaries of the ischioanal fossa. (W&B 531-532)Officially, the perineum is the outlet of the pelvis. (Used more loosely, it can refer to the area of skin between the anus and the posterior part of the external genitalia.) It is diamond-shaped, and can therefore be divided into two isosceles triangles by a line drawn between the ischial tuberosities. The anterior, or urogenital triangle has as its apex the pubic symphysis, with the ischiopubic rami as equal sides, and our imaginary line as the base. The posterior, or anal triangle is upside-down, with our line again as the base, the sacrotuberal ligaments as the equal sides, and the coccyx as the apex. (peri + inan ("to empty out" in Greek))
You really need to think about this in 3-D because, although drawn two-dimensionally from an inferior point of view it looks like the coccyx, anus, vagina, and pubic symphysis are all coplanar, they are not.
26. Describe the structure, contents, and course of the pudendal canal. (W&B 524-526, N 404, 405, 411, 413, TG 6-28A, 6-28B)The ischioanal fossa lies lateral to the anal canal and inferior to the pelvic diaphragm. Its boundaries are as follows:
- Superomedial: pelvic diaphragm (anterior recess extends superior or deep to the sphincter urethrae muscle)
- Medial: external anal sphincter muscle and anal canal
- Lateral: obturator internus fascia and ischial tuberosity
- Posterolateral: sacrotuberous ligament and gluteus maximus muscle (posterior recess extends superior to the gluteus maximus muscle)
27. Trace the branching pattern of the internal pudendal vessels and the pudendal nerve. (W&B 524-526, N 404, 405, 411, 413, TG 6-29A, 6-29B, 6-30A, 6-30B)The pudendal canal extends from the lesser sciatic foramen, where its contents enter the perineum, to the posterior edge of the perineal membrane. It contains the internal pudendal artery, internal pudendal vein, and the pudendal nerve.
28. Differentiate between the internal and external anal sphincters in structure and function. (W&B 530, 537, N 391A, 391B, 392, 393, TG 6-15A, 6-15B, 6-16)The internal pudendal artery gives off the following branches. The internal pudendal vein receives analogous tributaries.
- Within pudendal canal:
- inferior rectal artery: supply to lower rectum and anus
- perineal artery: supply to bulbospongiosus muscle and ischiocavernosus muscles, as well as posterior scrotal or posterior labial artery to supply the skin of the respective structures
- Within urogenital triangle:
- artery of the bulb of the vestibule (in females) or artery of the bulb of the penis (in males): supply to respective structures
- deep (central) artery of clitoris (in females) or deep (central) artery of the penis (in males) - within corpus cavernosum of appropriate structure
- dorsal artery of clitoris (in females) or dorsal artery of penis (in males): runs entire length of appropriate structure, sending branches to corpus cavernosa and terminate in branches to glans and prepuce.
The pudendal nerve has the following branches:
- Within pudendal canal:
- inferior rectal nerves: supply to external sphincter ani muscle and skin of anus
- perineal nerve: gives off posterior labial nerve (in female) or posterior scrotal nerve (in male), which supplies the skin of the perineum - also gives off the deep perineal nerve, which supplies motor innervation to all of the muscles of the urogenital triangle.
- Within urogenital triangle:
- dorsal nerve of clitoris (in female) or dorsal nerve of penis (in male): supply to appropriate structure
29. Differentiate between male and female urethrae. (W&B 542-543, N 369, 379, 384, 385, TG 6-08A, 6-08B, 6-09A, 6-09B, 6-10A, 6-10B)
- internal anal sphincter muscle: involuntary. It surrounds the superior 2/3 of anal canal. The internal anal sphincter muscle is a thickening of circular muscle that has parasympathetic innervation. It is contracted most of the time to prevent leakage of fluid and/or feces.
- external anal sphincter muscle: voluntary. It surrounds the superior 2/3 of anal canal as well, wrapped around the internal anal sphincter muscle. It constricts anal canal, but can be relaxed on command for the purpose of defecation.
30. Identify the components of the external genital organs and give the homologues in each of both sexes. (W&B 543-551, 403-413, N 379A, 379B, 382A, 382B, 418A, 418B, TG 6-25A, 6-25B, 6-27A, 6-27B)The female urethra is about four centimeters long and is entirely "membranous urethra". The male urethra is longer than the female urethra, and is divided into three parts: membranous, prostatic, and penile (spongy) urethra. (See Pelvis & Pelvic Viscera Dissector Answers.)
31. Describe structure and function of the erectile bodies. (W&B 520-523, 527-528, N 379A, 379B, 381, 382A, 382B, TG 6-27A, 6-27B, 6-32)
Female Male vestibular bulbs corpus spongiosum greater vestibular glands bulbourethral glands urethral and paraurethral glands prostate gland glans clitoris glans penis prepuce of clitoris prepuce of penis corpus of clitoris corpus (shaft) of penis labia minora penoscrotal raphe labia majora scrotum 32. Trace the nerve and blood supply to the external genital organs. (W&B 524-525, N 404, 405, 411, 413, TG 6-29, 6-30A, 6-30B)The three primary erectile bodies of the penis are the two corpora cavernosa and the corpus spongiosum. These structures are surrounded by a dense tunica albuginia such that, when they are engorged with blood, the penis becomes erect. The glans penis, the expanded cap of the corpus spongiosum, remains more malleable during erection because it has a much thinner tunica albuginea than the rest of the components of the penis.
The corpora cavernosa are rooted in the perineum by two crura of the penis. Each crus is attached to the ischiopubic ramus. The corpus spongiosum is rooted as the bulb of the penis, which is attached to the perineal membrane, and receives the membranous urethra as it transverses the membrane.
There are homologous structures in the female. The clitoris contains corpora cavernosa as its erectile tissue. Like in the male, each crus is attached to the ischiopubic ramus and perineal membrane. Instead of a corpus spongiosum, the female has two vestibular bulbs, which lie along the sides of the vestibule, and also expand as the glans clitoris to cap the distal ends of the corpora cavernosa.
34.Trace the lymphatic drainage of the perineum. (N 406, 407, 408A, 408B, TG 6-33, 6-34)The nerve supply to the external genital organs is via the pudendal nerve, which gives off the dorsal clitoral or penile nerve, and also gives off the perineal nerve, which in turn gives off posterior labial or posterior scrotal nerves and the deep perineal nerve supplying all of the muscles of the urogenital triangle.
The internal pudendal artery gives off the dorsal artery of the clitoris or penis and the deep artery of the clitoris or penis as terminal branches. It also gives off an artery to the bulb of the vestibule (in females) or an artery to the bulb of the penis (in males). The perineal artery gives off a posterior labial or posterior scrotal artery.
- perineum and external genitalia: drain to superficial inguinal nodes
- anal canal: superior part drains to internal iliac nodes, inferior part drains to superficial inguinal nodes
- testes: lymphatic vessels run with the spermatic cord, terminating in the lumbar nodes
Cultural enrichment: Check out these sections from the 1918 version of Gray's Anatomy of the Human Body! Some of the terms are (of course) out-of-date, but the illustrations are timeless.
Questions and Answers:
23. Note the difference between male and female in the subpubic angle, the angle formed by the subpubic arch. What are other sex differences in the pelvic skeleton? (W&B 571-573, N 354, TG 6-05A, 6-05B, 6-05CD, 6-05EF)27. On the sagittally-sectioned female specimen, trace the peritoneum from the ventral abdominal wall; examining the vesicouterine pouch and its manner of reflection from the bladder to the uterus. Onto what part of uterus does it reflect? (N 378, TG 6-08A)
Structure/Section Female Male pelvic inlet oval and rounded heart-shaped pelvic outlet large small pubic arch and subpubic angle wide narrow iliac wings flared less flared 28. Trace the peritoneum across the uterus and define the rectouterine pouch. Note peritoneum on the posterior wall of the vagina. From what point does the peritoneum reflect to the rectum? What is the significance of this? (N 360, TG 6-08A)The peritoneum on the superior surface of the bladder reflects onto the uterus at the isthmus, just superior to the cervix.
29. Within the broad ligament, locate the ovarian ligament and the round ligament of the uterus. Consider development and continuities of these structures. (N 367, 420, TG 6-11, 6-12)The peritoneum of the rectouterine pouch lies in contact with the posterior fornix of the vagina. This allows incisions, punctures, or lacerations of the posterior fornix of the vagina to open the peritoneal cavity. (This is often how eggs are harvested these days.)
30. Locate and define the peritoneal fold called the suspensory ligament of the ovary. What does it contain? (N 374, 400, TG 6-11A, 6-11B, 6-12)The proper ovarian ligament and the round ligament of the uterus are both remnants of the gubernaculum. They are continuous with one another where they contact the lateral surface of the uterus inferior to the uterine tube.
31. Strip the peritoneum from the suspensory ligament of the ovary on one side and trace the ovarian artery and vein. What are their sources? (N 400, TG 5-34)The suspensory ligament of the ovary contains ovarian vessels, autonomic nerves, lymphatics, and extraperitoneal connective tissue.
32. What is the complete area of distribution of the ovarian artery? (N 400, TG 6-11B, 6-12)The ovarian artery branches from aorta. The right ovarian vein drains to inferior vena cava. The left ovarian vein drains to left renal vein. (This is analogous to testicular vessels in males.)
33. Locate a ureter. Note its relation to uterine artery. Trace it to the bladder and posteriorly to the brim of the pelvis, noting course, relation to peritoneum, and blood supply. (N 400, TG 6-11B, 6-17)The ovarian artery supplies the ovary, mesovarium, and infundibulum of the uterine tube.
34. Trace the round ligament from the uterus to the deep inguinal ring. Where does it attach? (N 369, TG 6-07A, 6-11B, 6-12)The ureter passes over the pelvic brim just medial to the ovarian vessels, usually at the bifurcation of the common iliac artery. The ureter then descends and passes anteriorly within the pelvis. It is crossed superiorly by the uterine artery ("bridge over water") before it turns medially to enter the posterior wall of the bladder.
35. What structures support the uterus? (N 369, TG 6-13E)The round ligament of the uterus attaches to the lateral surface of uterus, below and anterior to the intramural portion of the uterine tube. It helps to hold the fundus of the uterus forward (anteverted).
36. Examine the vagina and the structure of its wall. Consider differences between the vagina and the vestibule of the vagina. (N 370, TG 6-08, 6-11, 6-12, 6-13)The round ligament of the uterus helps to hold the uterus in an anteverted position superior to the bladder. The cardinal ligaments and the endopelvic fascia around the uterine vessels helps to fix the cervix in place, as do the rectouterine ligaments. Even the broad ligament lends a slight amount of support to the uterus. (Anterversion of the uterus seems to be key, since retroversion is associated with prolapse of the uterus into the vagina. See #12 above.)
37. Examine the intravaginal cervix, the ostium of the uterus, and fornices of the vagina. Note relations to urethra, bladder, and rectum. What is the significance? (N 360, 370, 371, TG 6-08, 6-11, 6-12, 6-13)The vestibule of the vagina is the cleft between the paired labia minora. The vagina proper extends from the hymen or hymeneal caruncles at the vaginal orifice superiorly to the cervix of the uterus. Its wall is relatively muscular and covered with mucosa.
38. Explore the female urethra, noting length, sphincter muscle, and relation to vagina. Note specifically the relation of the orifice to the anterior vaginal wall. What is the significance? (W&B 549, N 383, 379, TG 6-08, 6-10)See descriptions of peritoneum, urinary apparatus, and vagina above.
39. Define the ampulla of the ductus deferens. Is it covered by peritoneum? (N 361A, 361B, 384A, 384B, TG 6-14)The urethra is about four centimeters long. It is homologous to male prostatic/membranous urethra. Its orifice is within the vestibule of the vagina, immediately in front of the vaginal orifice.
40. What is the rectovesical pouch? (N 361A, 361B, TG 6-08)The ductus deferens is covered by peritoneum, but its ampulla is not. The upper end of the seminal gland may contact peritoneum, otherwise it is inferior to the peritoneum lining the rectovesical pouch.
41. Where does the transition of the epididymis to the ductus deferens occur? (N 390, TG 6-32)The rectovesical pouch is the reflection of peritoneum between the rectum and the bladder. This of course only occurs in males.
9. Locate the anterior division of the internal iliac artery and note how it terminates by dividing into the inferior gluteal and the internal pudendal arteries. These exit the pelvis below the lower border of the piriformis muscle. What are other relations? (N 402, 403A, 403B, 502, TG 3-29, 6-17A, 6-17B)It occurs at the tail of the epididymis on the posteroinferior aspect of the testis.
The internal pudendal and inferior gluteal (the larger of the two) arteries are terminals of the anterior division of the internal iliac artery. They arise from a common trunk either within or outside the pelvis. The internal pudendal artery exits the greater sciatic foramen between the piriformis and coccygeus muscles, crosses the iliac spine to pass through the lesser sciatic foramen, and enters the pudendal canal. The inferior gluteal artery passes between the second and third sacral nerves to leave the pelvis below the piriformis muscle.10. Do you have an "aberrant obturator artery", which arises from the inferior epigastric artery and accompanies the obturator nerve?An aberrant obturator artery takes its origin from the inferior epigastric or, rarely, from the external iliac itself. It would descend along the brim of the pelvis to the obturator foramen.11. Locate the sympathetic trunk entering the pelvis along the medial border of the pelvic sacral foramina. Note number of ganglia, gray rami communcantes, and sacral splanchnic nerves. (N 410, 412, TG 8-18, 8-20)Both sympathetic trunks descend on the anterior surface of the sacrum in the extraperitoneal connective tissue. There are usually four ganglia in the sacral region, one opposite the upper three sacral segments and one beneath the fourth and fifth segments of the sacrum. The two trunks typically unite over the coccyx to form the "ganglion impar". Sacral splanchnic nerves are slender fibers leaving the anterior surface of the sacral sympathetic trunk ganglia to enter the inferior hypogastric plexus on the sides of the rectum. Gray rami communicantes also leave the lateral side of the sacral sympathetic trunk to reach the sacral ventral primary rami as they emerge from the anterior sacral foramina.12. How many pelvic splanchnic nerves are there? (N 410, 412, TG 8-19, 8-21)The pelvic splanchnic nerves represent the sacral portion of the craniosacral outflow or parasympathetic portion of the autonomic nervous system. The pelvic splanchnic nerves spring from the ventral rami of the second, third, and fourth sacral nerves. The contribution from the third sacral nerve is usually the largest. From three to ten strands of nerves pass forward and become incorporated into the inferior hypogastric plexus.13. What is the puborectalis muscle? What is its significance? (N 367A, 367B, 368, 369, 370, TG 6-21A, 6-21B, 6-22, 6-23A, 6-23B)The puborectalis muscle is the most medial portion of the levator ani muscle. It passes around the terminal rectum to form the puborectal sling, which kinks the anorectal junction forward to assist in maintaining fecal continence. This muscle marks the transition from rectum to anus.14. Define the urogenital hiatus. What does it transmit? (N 367A, 367B, 368, 369, 370, TG 6-21A, 6-21B, 6-22, 6-23A, 6-23B)The passage (transmission) of the urethra/vagina and anus through the pelvis requires a separation of the two halves of the pelvic diaphram in front of the rectum. This is the urogenital hiatus.11. Do you find muscular (deep) branches of the perineal nerves? (N 411, 413, TG 6-30A, 6-30B)The deep perineal nerve innervates all of the muscles of the urogenital triangle via slender branches that may be difficult to locate.12. What is the source and drainage of the deep dorsal vein of the clitoris/penis and the dorsal veins and arteries of the clitoris/penis? (N 265, 383, 359, 404, 405, 381, TG 5-34, 6-10, 6-23, 6-27, 6-29)13. What is the function of the perineal membrane? (N 404, 405, 411, 413, TG 6-27A, 6-27B, 6-28A, 6-28B)The deep dorsal veins drain into the vesical venous plexus. The "normal" dorsal veins drain into the superficial external pudendal vein. The dorsal arteries come from the internal pudendal arteries.
This membrane covers the anterior part of pelvic outlet. It aids in support of the pelvic viscera and as an attachment for perineal structures. It is pierced by the arteries of the erectile bodies and the dorsal arteries and nerves of the clitoris or penis.14. What is the source of the deep (central) artery of the clitoris/penis? (N 404, 405, 6-29A, 6-29B)This artery is a branch of the internal pudendal artery.15. What gland is embedded in the sphincter urethrae muscle in males? (N 385A, 384B, 379A, 379B)In males, the bulbourethral glands (Cowper's glands) are embedded in the external urethral sphincter muscle. In females, the greater vestibular gland is the homologous structure, but it is not associated with the sphincter urethrae muscle. (The greater vestibular glands lie posterior to the vestibular bulb, under the cover of the bulbospongiosus muscle.)